 It seemed so easy when Sgt. Joe Friday said it on Dragnet. Why do we have so much difficulty in practicing medicine that way, based on evidence, on facts? Here are some of the barriers, as I see them.
It seemed so easy when Sgt. Joe Friday said it on Dragnet. Why do we have so much difficulty in practicing medicine that way, based on evidence, on facts? Here are some of the barriers, as I see them.
1. Evidence generation. This seems obvious, but evidence-based practices requires, well, evidence. In many fields, especially pediatrics, there is a serious lack of evidence to support even treatments that are widely used. One issue is lack of funding. NIH funding, even before it began to decline due to the federal budget sequester, often goes preferentially to basic science rather than clinical trials, and to adult trials that address common, high-impact conditions. While regulations about inclusion of children in research, the Better Pharmaceuticals for Children Act, and FDA incentives for industry to do perform pediatric trials to support patent extension have helped, funding for pediatric patient-oriented research continues to lag. Pediatric trials are also difficult to conduct. Many childhood diseases are sufficiently rare that they can only be studied in the context of multicenter trials, which are logistically challenging and more expensive to conduct (typically exceeding the level requiring additional scrutiny at NIH).
Nevertheless, generating evidence is absolutely critical. When we do systematically evaluate treatments, as a study in Mayo Clinic Proceedings shows, the results often fail to support established practices. Of 363 comparative trials of established practice reviewed, 40% showed that a standard practice was ineffective or harmful, 38% reaffirmed established practice, and the rest were inconclusive.
2. Evidence dissemination. Even when studies are done to critically evaluate a diagnostic test or treatment, the results may not be widely disseminated. Publication bias – the tendency for authors to prefer to submit, or for journals to prefer to publish, studies with positive results, has been well described. The reasons may include profit motive (for industry sponsored trials), legitimate concerns about negative results from underpowered studies, or sheer laziness. The requirements by major journals to register trials before they begin as a condition for publication was supposed to help minimize publication bias, or at least enable its detection. But a study in PLoS found that only 46% of reportedly completed trials listed in ClinicalTrials.gov had been published. Publication rates were lowest for industry sponsored studies (40%), followed by 47% for government funded studies and 56% for non-government, non-industry supported studies.
And of course, there is the sheer volume of stuff to read. Medical and scientific journals have exploded in number; it is nearly impossible for a practicing provider to keep up with the literature.
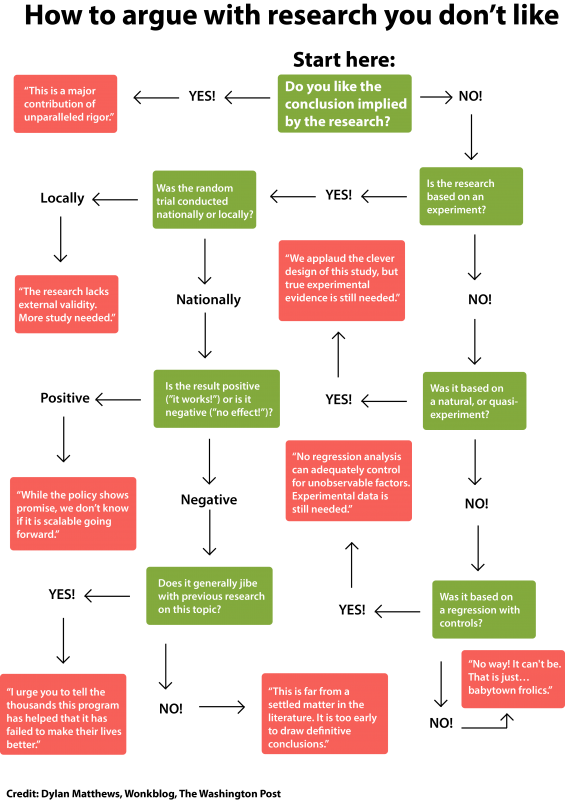
3. Knowledge translation. Even when results are disseminated, the time for new findings to be adopted into widespread clinical practice has lagged. It has been reported that innovations can take 10 years to become commonly used. Reasons include entrenched interest in the status quo (which does not only apply to for profit industry – evidence questioning the utility of a procedure, for example, may threaten the specialists who perform it), and sheer inertia. Physicians are naturally skeptical, and often question the data when it does not conform to their pre-existing beliefs. This figure illustrates the gauntlet a study must run before it can be accepted as the basis for a practice change.
Evidence-based medicine has the potential to reduce the excessive variation in practice that has been widely described. The goal is not to eliminate variation, only to minimize unnecessary variation. Different patients with the same disease will differ in their exact biological needs as well as their preferences; these differences must be understood and accounted for. But their management should not be based on which part of the country a doctor happened to train in, or what year she graduated from medical school, or her Myers-Briggs personality type. We expect the legal system to operate based on the facts – the medical system should do no less.